Sykor iFrax: The Continuation of the Search for the Fountain of Youth (and Beauty)
The world of aesthetic medicine has changed in the past two decades. First, most aesthetic procedures are being performed by non-surgeons. Second, side effects, adverse events and patient downtime have become major issues. As medical technology moved from the earliest “continuous wave” carbon dioxide (CO2) lasers to pulsed CO2 lasers and then to pigment-based lasers and intense pulsed light, treatments were also developed for treating birthmarks and tattoos and for performing hair removal. Gradually, cleared indications for lasers have widened and devices have emerged for the successful treatment of leg veins and facial rejuvenation. More recently, devices have been developed using radiofrequency (RF) and ultrasound. The search for the “Holy Grail” continues.

Everyone is searching for devices that will produce facial rejuvenation with less downtime and risk of unwanted side effects (i.e., post inflammatory hyperpigmentation or “PIH”) than is associated with surgery or other methods. Market analysis and current statistics show continual growth in the field of medical aesthetic devices, with an average increase of 7.3 percent every year over the past 5 years. A medical practice treating patients with devices requires reliable devices that will provide numerous treatment sessions at a low cost. Many experts believe that up to now the efficacy of aesthetic devices has remained far from reaching clinical results comparable to surgery. For a device to be successful, it has to “pass” a certain barrier on its way to satisfactory aesthetic results. This barrier can be divided into four distinct checkpoints:
1. Physical stage: A successful device must be based on sound physical principles.
2. Biology: Energy delivered to the tissues can spread and fail to reach its target with sufficient energy to produce the desired result (i.e., coagulation, etc.). The human biological system is very complex and includes many unknown and personal variables.
3. Clinics: A higher barrier in the way of patient satisfaction is true clinical evidence of a device’s efficacy. Much of the published data of the commercial devices on the market show impressive photographs but ignore true statistics, patient selection factors, and other critical factors.
4. Patient satisfaction: True evidence of any aesthetic intervention is the final “product”—patient satisfaction. Patient satisfaction is highly dependent on the clinical results, but also on the expectations the patient has in mind. Social factors and marketing and pricing of the procedure are also important. Patients may willing to accept less dramatic results for less risk and downtime, but those results should also be seen by the patients and society.
In the past, the Food and Drug Administration and the European Conformity clearance or “approval” of medical devices was generally given after only safety was proven. However, today, true efficacy is required, and sound clinical studies have to be performed after institutional review board approval. Today, many experts believe that believe that in many cases aesthetic surgery will be replaced by non-invasive and minimally-invasive devices attempting to produce comparable results. Since its introduction in the mid 1980s, technologies and procedures geared toward “rejuvenating the skin” have continued to evolve. Carbon dioxide skin resurfacing lasers gave way to less invasive erbium devices, which in turn led to non-invasive “photorejuvenation” systems. Fractional technology was introduced in 2003 and has quickly become the new standard. Now including both ablative and non-ablative systems using both light and RF technologies, fractional systems offer further improvements in their ability to deliver higher levels of power into the skin for a more profound result with less unwanted damage to the skin.
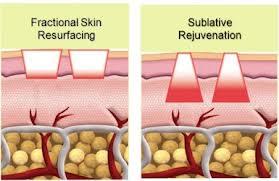
Developers continue to advance skin rejuvenation technology. In 2009, “sublative RF rejuvenation” (SRFR) was introduced. SRFR delivers RF energy to the skin in a fractional manner that offers significant benefits over prior methods. First, because SRFR results in most of the “treatment effect” occurring beneath the epidermis and at sublative levels of heating, it simulates the effects of ablative/coagulative lasers but results in less downtime and pigmentation risk because the epidermis is essentially bypassed. Practitioners testing SRFR systems report achieving dramatic results in skin tightening, wrinkle reduction and scar softening for patients of all skin types, with minimal discomfort and side effects. This is attributed largely to the unique “pyramid shape” of the treated area (with the large bottom section reaching the dermis), as shown below, compared to a uniform cylindrical column of tissue damage created by conventional fractional systems (also shown below).
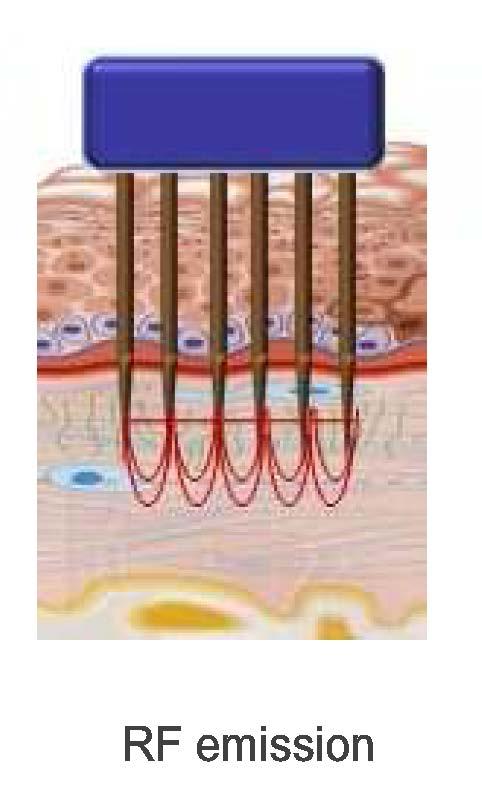
This “pyramid shape” energy delivery allows the usage of more targeted energy that creates a greater temperature rise in the deeper dermal skin layers. In comparison, highly ablative fractional treatments are often not recommended for darker skin types due to extensive impact at the epidermal skin level. More recently, even more advanced fractional RF devices—such as the iFRAX System– have been introduced that incorporate large numbers of specially designed, fine micro-needles which penetrate the skin causing both physical micro-trauma and with each puncture together with simultaneous micro-delivery of fractional RF energy. These FRF devices deliver RF energy to the skin via stainless steel needles. Since stainless steel has significantly higher electrical conductivity than human skin, the RF energy travels directly down each needle and the between the alternately positive and negative needles (as shown below) with little or no energy being delivered to the skin (except at the target point) due to the much higher electrical impedance of the skin. As a result, only the targeted tissue at the precise level to which the needles are inserted is heated. By setting the needles to be inserted 1 mm or deeper, you can completely bypass the epidermis and avoid complications for darker-skinned patients.